PANDEMIC PREPAREDNESS
AVIAN FLU FACTS
**********************
Pandemic Planning and Preparedness
Testimony of Julie L. Gerberding, MD, MPH
Director – Centers for Disease Control and Prevention
Before the Subcommittee on Health, Committee on Energy and Commerce
U.S. House of Representatives
May 26, 2005
Mr. Chairman and members of the Subcommittee, I am pleased to be here today to describe planning and preparedness for an influenza pandemic, including the potential threat posed by the H5N1 avian influenza virus currently in Asia. Department of Health and Human Services Secretary Mike Leavitt has made influenza pandemic planning and preparedness one of his top priorities; and each agency within the Department is working together to prepare the United States for a potential threat to the health of our nation.
I will discuss steps the Centers for Disease Control and Prevention (CDC) is taking with many partners both domestically and globally. The strength and flexibility of CDC and other components of the public health system are vital assets as the United States sharpens its readiness for an influenza pandemic. Although we have made significant progress, more work is needed, particularly in the areas of surveillance capacity and response, and the development of potential vaccines. Increased public awareness and understanding about infection control, containment, and other actions also are important in preparation for an influenza pandemic.
Pandemics in Perspective
Seasonal influenza causes an average of 36,000 deaths each year in the United States, mostly among the elderly and nearly 200,000 hospitalizations. In contrast, the actual severity and impact of the next pandemic, whether from H5N1 or another influenza virus, cannot be predicted. However, modeling studies suggest that, in the absence of any control measures, such as vaccination, a “medium-level� pandemic in the United States could result in 89,000 to 207,000 deaths, between 314,000 and 734,000 hospitalizations, 18 to 42 million outpatient visits, and another 20 to 47 million people being sick. Between 15 percent and 35 percent of the United States population could be affected by an influenza pandemic, and the economic impact in our country alone could range between $71.3 and $166.5 billion. A public health response to a disease of this magnitude involves numerous challenges.
- A pandemic can occur any time during the year and can last much longer than seasonal influenza.
- In more advanced pandemic phases, the capacity to prevent or control transmission of the virus can become extremely difficult.
- Although the primary concern at present is the H5N1 avian influenza strain in Asia, an outbreak leading to a pandemic can occur anywhere in the world and may derive from viral strains of influenza other than H5N1.
- Comparing the onset and spread of the next pandemic to those of the 20th century is problematic for many reasons, including changes in population and social structures, medical and technological advances, and the increase in international travel.
- With zoonotic diseases such as avian influenza, there is a need for coordination with the animal health community.
The Current Situation in Asia
For an influenza virus to cause a pandemic, it must meet three major criteria: (1) possess a new surface protein to which there is little or no pre-existing immunity in the human population; (2) be able to cause illness in humans; and (3) have the ability for sustained transmission from person to person. So far, the H5N1 virus has met two of these three criteria, but it has not yet shown the capability for sustained transmission from person to person.
Concerning this third point, it is important to keep in mind the close relationship of viral infections in animal hosts and those in humans. Ongoing dialogue between agricultural and public health officials is extremely important for the careful, consistent surveillance necessary in both animal and human populations. Although the present avian influenza H5N1 strain in Asia does not yet have the capability of sustained person-to-person transmission, chicken-to-human transmission has occurred, and in at least one cluster, limited person-to-person transmission has been identified. As of May 19, 2005 the World Health Organization (WHO) had confirmed 97 cases of H5N1 influenza in humans since January 28, 2004, with a case fatality rate of 55 percent. The World Organization for Animal Health (OIE) confirmed, as of May 13, 2005, that H5N1 had been found in animals from nine Asian countries in 2004 and 2005, with especially large outbreaks among animals in Vietnam and Thailand. Millions of domestic birds have been culled in attempts to stop the spread of the virus among animal populations.
Although human case fatality rates seem to have gone down somewhat since February 2005, CDC, WHO, and other partners are still quite concerned for several reasons. The H5N1 strain now appears to be endemic in poultry and other birds in a number of Asian countries, signaling a potential long-term threat of mutation and reassortment with other viral strains. Recent studies have found that ducks carry the H5N1 strain asymptomatically, making it difficult to monitor the magnitude of transmission from ducks to other species. Confirmation that H5N1 also has been transmitted to mammals is a particular concern, because of the increased potential of the strain to reassort with other strains already common to humans and other mammals. Studies have documented highly pathogenic H5N1 in pigs, tigers, and leopards in Asia. Difficulties in implementing effective in-country surveillance, including enhancing the training of laboratorians, epidemiologists, veterinarians, and other professionals, inhibit the type of comprehensive reporting that is essential to monitor H5N1 and other strains of highly pathogenic avian influenza. Finally, changes in the epidemiology of the infections, such as decreasing mortality rates, could indicate changes that make the viruses better adapted to humans. Additional studies and research are needed to better understand the current situation and how the viruses may be changing.
Responding to a Pandemic
An effective response to an influenza pandemic requires highly collaborative planning, implementation, and flexibility in resolving issues at many levels. The Department of Health and Human Services (DHHS) is leading the coordination of preparedness efforts through its Pandemic Influenza Response and Preparedness Plan, which was released in draft form in August 2004 for public comment and is under revision. In addition, states are either developing pandemic influenza plans or revising existing plans to reflect new information and data. Key elements of these plans include surveillance, infection control, use of antiviral medications, community containment measures, vaccination procedures, communications, and ability to sustain essential services in times of widespread illness. Similar elements inform a plan that CDC is developing, that will provide detailed guidance and materials to states and localities and will complement the DHHS plan. CDC also will take the lead in working with the Advisory Committee on Immunization Practices and the National Vaccine Advisory Committee to prioritize recommended target groups for use of antiviral medications and vaccines during a pandemic when supplies are limited.
Once a pandemic strain starts circulating in the United States, isolation precautions for persons who are ill and quarantine for persons exposed may need to be considered to limit the early spread of pandemic influenza, particularly before a vaccine becomes available. Measures such as these will require a multi-level, multifaceted, staged process, such as evaluating all ill travelers arriving from affected areas. On April 1, 2005 the President amended Executive Order 13295, adding influenza caused by novel or reemergent influenza viruses that are causing, or have the potential to cause, a pandemic to the list of quarantinable diseases. CDC has implemented a series of travel notices to minimize the potential for outbreaks to extend to wider geographic areas. CDC also has expanded the number and capacity of its quarantine stations at major ports of entry into the United States. As with any quarantine, such activities need to be undertaken judiciously to minimize adverse impacts on civil liberties. Vaccination is the best long-term strategy for influenza prevention and control, both during annual outbreaks and a pandemic; antiviral medications provide an earlier, secondary line of defense. Other measures may help control the spread of influenza in a pandemic situation, such as isolation of ill persons and quarantine of healthy exposed persons. Comprehensive preparedness for annual influenza outbreaks is a vital component of an effective response to pandemic influenza, although pandemic planning will require additional preparation activities. Surveillance
The United States, working domestically and with global partners, needs to expand the scope of early-warning surveillance activities used to detect the next pandemic. We cannot estimate the amount of time from first detection in another country to peak disease in the United States, but it could be a matter of months or less. Time will be of the essence in making sure we can produce, test, and administer vaccine as quickly as possible. It will take several months for the first dose of pandemic vaccine to be ready and longer to manufacture enough to vaccinate the entire U.S. population. Therefore, vaccine will be in short supply at the start of the pandemic. Under the most favorable conditions, by the time the first dose of vaccine would be given to the first person, many others will have already become ill or died. For this reason, surveillance to monitor ongoing changes in the H5N1 strain of avian influenza currently causing human infections and to monitor for other viruses with pandemic potential is needed to develop prototype vaccine candidates as quickly as possible. Further, because such a pandemic strain can arise anywhere, at any time, expanded global surveillance capacity is needed.
The outbreaks of avian influenza in Asia have highlighted several gaps in disease surveillance globally that the United States must help address to improve our ability to prepare for an influenza pandemic. These challenges include: (1) lack of infrastructure in many countries for in-country surveillance networks; (2) need for increased training of laboratory, epidemiologic, and veterinary staff; and (3) resolution of longstanding obstacles to rapid and open sharing of surveillance information, specimens, and viruses among agriculture and human health authorities in affected countries and the international community. CDC and HHS have made significant progress in the past year toward enhancing surveillance in Southeast Asia. This initiative needs to continue at both national and international levels if we are to expand geographic coverage and develop an adequate capacity to conduct effective surveillance. These efforts, in turn, will increase our ability to detect new variants earlier, make more informed vaccine decisions for yearly epidemics, and build an “early warning system� for new viruses that may cause a pandemic. With the ever-present threat of the emergence of a new pandemic strain, we need to know what is happening in the backyards of Southeast Asia, as well as elsewhere throughout the world. Year-round, world-wide surveillance for infections of humans with new strains of influenza is essential for us to prepare for the next pandemic, as well as for next year’s epidemic. Recently, the Congress passed and the President signed an FY 2005 Emergency Supplemental Appropriations Act for Defense, the Global War on Terror, and Tsunami Relief, which included $25 million in international assistance funds to prevent and control the spread of avian influenza in Southeast Asia. These funds will support human surveillance, laboratory capacity, and enhanced knowledge of state-of-the-art avian influenza laboratory and field techniques in Southeast Asia.
In the past year, CDC has considerably improved domestic surveillance, adding two new major components to our surveillance system. We worked with the Council for State and Territorial Epidemiologists (CSTE) to make confirmed pediatric deaths from influenza nationally notifiable, and we implemented hospital-based surveillance for influenza in children at selected sites. To further improve our understanding of the impact of influenza on severe outcomes, such as hospitalization, we are working with the CSTE to make all laboratory confirmed influenza hospitalizations notifiable. We have issued interim guidelines to states and hospitals to enhance surveillance for potential cases of people infected by avian influenza on several occasions and these enhancements continue. CDC also set up special laboratory training courses for identification of avian influenza using rapid molecular techniques. So far, professionals from 48 states and Washington D.C. have been trained. However, to be as prepared as possible for a pandemic, we are working to do much more in the domestic surveillance arena. The United States is working to: (1) ensure that states have sufficient epidemiologic and laboratory capacity both to identify novel viruses throughout the year and to sustain surveillance during a pandemic; (2) improve reporting systems so that information needed to make public health decisions is available quickly; (3) enhance systems for identifying and reporting severe cases of influenza; (4) develop population-based surveillance among adults hospitalized with influenza and (5) enhance monitoring of resistance to current antiviral drugs, to guide policy for use of scarce antiviral drugs.
Managing the Vaccine Supply
During an influenza pandemic, the presence of U.S.-based manufacturing facilities will be critically important. The pandemic influenza vaccines produced in other countries will likely not be available to the US market as those governments may prohibit export of the vaccines produced in their countries until their domestic needs are met. However, the vaccine manufacturing system in the United States is fragile. Currently, there are only three influenza vaccine manufacturers producing vaccines for the US market, and only one produces its vaccine entirely in the United States.
During the past several years, CDC and other DHHS agencies have developed several new strategies to address annual influenza outbreaks, including the support of enhanced vaccine production, and have worked to ensure a better match of vaccine distribution to the populations in greatest need. Public demand for influenza vaccine on a yearly basis needs to be both stabilized and increased, so that companies will have a growing market to provide an incentive to increase production. These strategies include $40 million for purchasing influenza vaccine for the pediatric stockpile to protect against annual outbreaks of influenza, and $30 million will be used for contracts to expand the production of bulk single-strain influenza vaccine for use if needed during annual influenza season or possibly in a pandemic situation. In addition, the President is requesting $120 million in fiscal year 2006, an increase of $21 million, to encourage greater production capacity that will enhance the U.S.-based vaccine manufacturing surge capacity to help prepare for a pandemic and further guard against annual shortages.
The Department also appreciates the inclusion of $58 million in the FY 2005 Emergency Supplemental to procure additional influenza countermeasures for the CDC Strategic National Stockpile (SNS) in FY 2005. Currently, the SNS has enough oseltamivir (Tamiflu) capsules to treat approximately 2.26 million adults and oseltamivir (Tamiflu) suspension to treat more than 100,000 children. In addition, SNS contains enough rimantadine (Flumadine) tablets to treat up to 4.25 million people and enough rimantadine suspension to treat up to 750,000. It should be noted, however, that oseltamivir is the only antiviral at this time shown to be effective against the H5N1 avian influenza virus in Asia. In addition, SNS funds have been used to purchase approximately 2 million bulk doses of unfinished, unfilled H5N1 vaccine, although it is not yet formulated into vials nor is the vaccine licensed. Clinical testing to determine dosage and schedule for this vaccine began in April 2005 with funding from the National Institutes of Health.
DHHS also is supporting the development and testing of potential dose-sparing strategies to extend a given quantity of vaccine stock. Regarding annual influenza vaccination, there is an emerging consensus that it is desirable to expand vaccine coverage beyond the high priority groups for whom routine vaccination is already recommended. Discussions are under way to review the data that would be needed to consider broadening recommendations for influenza vaccination. CDC is developing strategies to increase informed demand for, and access to, influenza vaccine for persons who are currently recommended to be vaccinated each year. For example, according to a 2003 Institute of Medicine report, an estimated 8.2 million additional high-risk uninsured adults 18-64 years old warrant annual vaccination. We recognize that these at-risk persons need better access to vaccine during a pandemic as well as for seasonal influenza. Additionally, CDC, in conjunction with the Advisory Committee on Immunization Practices, is developing an internal set of possible influenza vaccine supply scenarios that may occur in future influenza seasons and during a pandemic. These scenarios range from worst-case to best-case situations and are an important part of CDC planning efforts. We are preparing recommendations, plans, and communication messages for any of the possible situations.
Conclusion
Although the present avian influenza H5N1 strain in Southeast Asia does not yet have the capability of sustained person-to-person transmission, we are concerned that it could. CDC is closely monitoring the situation in collaboration with the World Health Organization. CDC is using its extensive network of partnerships with other federal agencies, provider groups, non-profit organizations, vaccine and antiviral manufacturers, and state and local health departments to enhance pandemic influenza planning. Our responses to the annual domestic influenza seasons also will inform the nation’s planning and preparedness for pandemic influenza. The same laboratories, health care providers, surveillance systems, and health department plans and personnel guide both responses. These actions, in conjunction with increased public understanding about influenza, will help us all prepare for an influenza pandemic.
Avian Influenza Viruses
What’s Happening Now?
It is difficult to predict when the next influenza pandemic will occur or how severe it will be. Wherever and whenever a pandemic starts, everyone around the world is at risk. Countries might, through measures such as border closures and travel restrictions, delay arrival of the virus, but cannot stop it.
Health professionals are concerned that the continued spread of a highly pathogenic avian H5N1 virus across eastern Asia and other countries represents a significant threat to human health. The H5N1 virus has raised concerns about a potential human pandemic because:
- It is especially virulent
- It is being spread by migratory birds
- It can be transmitted from birds to mammals and in some limited circumstances to humans, and
- Like other influenza viruses, it continues to evolve.
Since 2003, a growing number of human H5N1 cases have been reported in Azerbaijan, Cambodia, China, Egypt, Indonesia, Iraq, Thailand, Turkey, and Vietnam. More than half of the people infected with the H5N1 virus have died. Most of these cases are all believed to have been caused by exposure to infected poultry. There has been no sustained human-to-human transmission of the disease, but the concern is that H5N1 will evolve into a virus capable of human-to-human transmission.
Avian Influenza Viruses
Avian (bird) flu is caused by influenza A viruses that occur naturally among birds. There are different subtypes of these viruses because of changes in certain proteins (hemagglutinin [HA] and neuraminidase [NA]) on the surface of the influenza A virus and the way the proteins combine. Each combination represents a different subtype. All known subtypes of influenza A viruses can be found in birds. The avian flu currently of concern is the H5N1 subtype.
Avian Influenza in Birds
Wild birds worldwide carry avian influenza viruses in their intestines, but usually do not get sick from them. Avian influenza is very contagious among birds and can make some domesticated birds, including chickens, ducks, and turkeys, very sick and kill them. Infected birds shed influenza virus in their saliva, nasal secretions, and feces. Domesticated birds may become infected with avian influenza virus through direct contact with infected waterfowl or other infected poultry, or through contact with surfaces (such as dirt or cages) or materials (such as water or feed) that have been contaminated with the virus. Avian influenza infection in domestic poultry causes two main forms of disease that are distinguished by low and high extremes of virulence. The “low pathogenic” form may go undetected and usually causes only mild symptoms (such as ruffled feathers and a drop in egg production). However, the highly pathogenic form spreads more rapidly through flocks of poultry. This form may cause disease that affects multiple internal organs and has a mortality rate that can reach 90-100%, often within 48 hours. The H5N1 virus is highly pathogenic.
Human Infection with Avian Influenza Viruses
“Human influenza virus” usually refers to those subtypes that spread widely among humans. There are only three known A subtypes of influenza viruses (H1N1, H1N2, and H3N2) currently circulating among humans. It is likely that some genetic parts of current human influenza A viruses originally came from birds. Influenza A viruses are constantly changing, and other strains might adapt over time to infect and spread among humans. The risk from avian influenza is generally low to most people, because the viruses do not usually infect humans. H5N1 is one of the few avian influenza viruses to have crossed the species barrier to infect humans, and it is the most deadly of those that have crossed the barrier.
Most cases of H5N1 influenza infection in humans have resulted from contact with infected poultry (e.g., domesticated chicken, ducks, and turkeys) or surfaces contaminated with secretion/excretions from infected birds. So far, the spread of H5N1 virus from person to person has been limited and has not continued beyond one person. Nonetheless, because all influenza viruses have the ability to change, scientists are concerned that H5N1 virus one day could be able to infect humans and spread easily from one person to another.
In the current outbreaks in Asia, Europe, and Africa, more than half of those infected with the H5N1 virus have died. Most cases have occurred in previously healthy children and young adults. However, it is possible that the only cases currently being reported are those in the most severely ill people, and that the full range of illness caused by the H5N1 virus has not yet been defined. Symptoms of avian influenza in humans have ranged from typical human influenza-like symptoms (e.g., fever, cough, sore throat, and muscle aches) to eye infections, pneumonia, severe respiratory diseases (such as acute respiratory distress), and other severe and life-threatening complications. The symptoms of avian influenza may depend on which virus caused the infection. Because these viruses do not commonly infect humans, there is little or no immune protection against them in the human population. If H5N1 virus were to gain the capacity to spread easily from person to person, a pandemic (worldwide outbreak of disease) could begin. No one can predict when a pandemic might occur. However, experts from around the world are watching the H5N1 situation very closely and are preparing for the possibility that the virus may begin to spread more easily and widely from person to person.
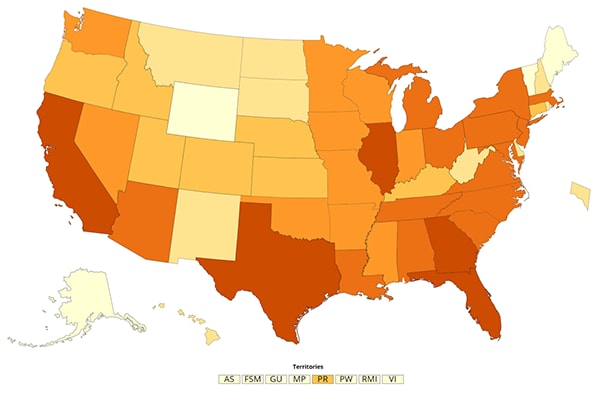
For the most current information about avian influenza and cumulative case numbers, see the map on this site’s home page.
For more information about human infection, see http://www.cdc.gov/flu/avian/gen-info/avian-flu-humans.htm
Vaccination and Treatment for H5N1 Virus in Humans
There currently is no commercially available vaccine to protect humans against H5N1 virus that is being seen in Asia, Europe, and Africa. A pandemic vaccine cannot be produced until a new pandemic influenza virus emerges and is identified. The U.S. Department of Health and Human Services (HHS), through its National Institute of Allergy and Infectious Diseases (NIAID), is addressing the problem in a number of ways. These include the development of pre-pandemic vaccines based on current lethal strains of H5N1, collaboration with industry to increase the Nation’s vaccine production capacity, and seeking ways to expand or extend the existing supply. We are also doing research in the development of new types of influenza vaccines.
Studies done in laboratories suggest that some of the prescription medicines approved in the United States for human influenza viruses should work in treating avian influenza infection in humans. However, influenza viruses can become resistant to these drugs, so these medications may not always work. Additional studies are needed to demonstrate the effectiveness of these medicines. The H5N1 virus that has caused human illness and death in Asia is resistant to amantadine and rimantadine, two antiviral medications commonly used for influenza. Two other antiviral medications, oseltamavir and zanamavir, would probably work to treat influenza caused by H5N1 virus, but additional studies still need to be done to demonstrate their effectiveness. The massive mortality due to the influenza epidemic in October of 1918 in Kansas. This is representative of what happened in every state in the nation.
What would be the Impact of a Pandemic?
A pandemic may come and go in waves, each of which can last for six to eight weeks. An especially severe influenza pandemic could lead to high levels of illness, death, social disruption, and economic loss. Everyday life would be disrupted because so many people in so many places become seriously ill at the same time. Impacts can range from school and business closings to the interruption of basic services such as public transportation and food delivery.
Pandemics Death Toll Since 1900
1918-1919
U.S….500,000+
Worldwide…40,000,000+
1957-1958
U.S…. 70,000+
Worldwide…1-2,000,000
1968-1969
U.S….34,000+
Worldwide…700,000+
A substantial percentage of the world’s population will require some form of medical care. Health care facilities can be overwhelmed, creating a shortage of hospital staff, beds, ventilators and other supplies. Surge capacity at non-traditional sites such as schools may need to be created to cope with demand. The need for vaccine is likely to outstrip supply and the supply of antiviral drugs is also likely to be inadequate early in a pandemic. Difficult decisions will need to be made regarding who gets antiviral drugs and vaccines. Death rates are determined by four factors: the number of people who become infected, the virulence of the virus, the underlying characteristics and vulnerability of affected populations and the availability and effectiveness of preventive measures.
How are We Preparing?
The United States has been working closely with other countries and the World Health Organization (WHO) to strengthen systems to detect outbreaks of influenza that might cause a pandemic. See Global Activities The effects of a pandemic can be lessened if preparations are made ahead of time. Planning and preparation information and checklists are being prepared for various sectors of society, including information for individuals and families. HHS and other federal agencies are providing funding, advice, and other support to your state to assist with pandemic planning and preparation. Information on state/federal planning and cooperation, including links to state pandemic plans, is available on this site. The federal government will provide up-to-date information and guidance to the public through the public media and this web site should an influenza pandemic unfold.
History of Pandemics
·Timeline of Human Flu Pandemics (National Institute of Allergy and Infectious Diseases)
See a chronology of significant dates in pandemic influenza history.
Pandemics and Pandemic Threats since 1900
Learn about the three pandemics and several “pandemic threats” that have occurred.
The Deadly Virus: The Influenza Epidemic of 1918 (National Archives and Records Administration)
View archival documents and photos from the era of the Great Pandemic of 1918.
The Great Pandemic of 1918: State by State
Read stories and anecdotes of the impact of the Great Pandemic in individual states.
The American Experience, Influenza 1918 (Public Broadcasting Service)
Read the history of “the worst epidemic the U.S. has ever known”
Influenza Pandemics of the 20th Century (Centers for Disease Control and Prevention)
Read about the worldwide (pandemic) outbreaks of influenza that occurred in the 20th century: in 1918, 1957, and 1968.
Swine Influenza A Outbreak, Fort Dix, New Jersey, 1976 (Centers for Disease Control and Prevention)
Find out how the Swine Influenza A Outbreak affected the health of the Fort Dix soldiers in 1976.
The Swine Flu Episode and the Fog of Epidemics (Centers for Disease Control and Prevention)
Read about the lessons learned from previous epidemics.
-(condensed from CDC public websites)